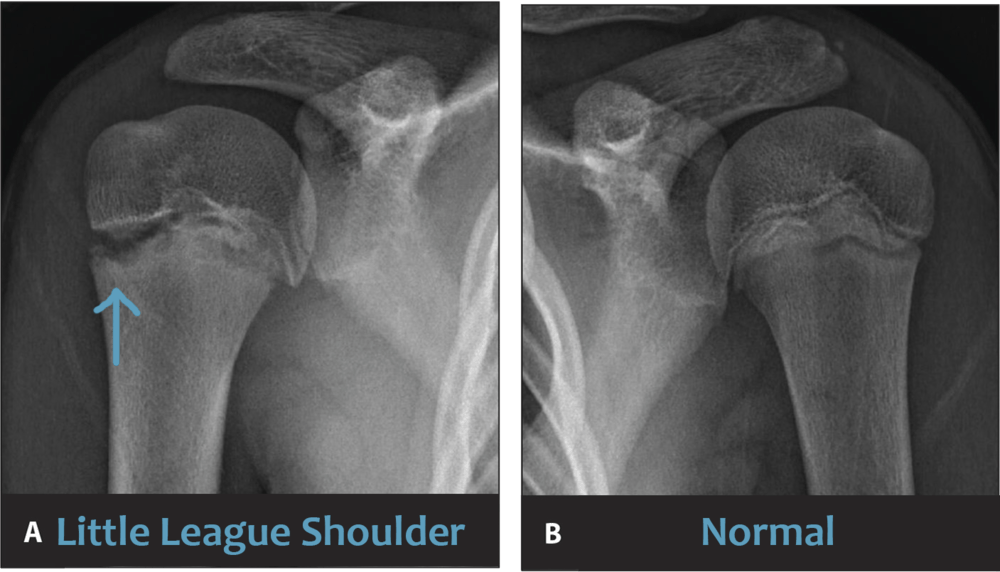
Little League shoulder is an overuse injury that affects young baseball players’ upper arm growth plate. The image below shows the widening of the upper arm growth plate in a young athlete with Little League shoulder. Pain in the shoulder or upper arm during throwing is the hallmark sign. In more severe cases, Little League shoulder pain is present during activities of daily living or even at rest.
Little League shoulder and Little League elbow are treated first with a period of rest. During this period of rest, physical therapy begins to improve strength and flexibility. Premature closure and fractures of the growth plate have been reported with Little League shoulder. However, these are rare complications. Most will eventually ‘‘outgrow’’ the condition with normal growth plate closure. However, some continue to experience pain during the preadolescent or adolescent years. In some athletes, this considerably limits participation and can even end their playing career.
Little League shoulder most commonly occurs in overhead athletes between the ages of 11 and 16 years. Thirteen years old is the most common age at which players move to a larger diamond. This requires a longer distance for pitches to cross home plate. Therefore, this is the period where coaches and parents should most closely monitor youth athletes for early signs of pain.
Read on to learn about the 5 keys to returning your already injured baseball player to play safely.
#1 Little League Shoulder is Occurring with Increasing Frequency
The increasing frequency of Little League shoulder is due to overuse and throwing with arm fatigue. This trend is due to greater numbers of pitchers participating in competitive leagues and doing so at increasingly younger ages.
Increased velocity is also a likely contributor. Year-round participation, participation on multiple teams in a season, the influence of private pitching coaches, and ‘‘showcase’’ events all contribute to increased stress to the maturing athlete. Coaches and parents must monitor players in accordance with Little League pitch count recommendations. Players should also take at least 3 to 4 months per year off from pitching.
#2 Little League Shoulder Treatment Always Includes Rest from Throwing

During the late portion of the arm-cocking phase of throwing, considerable forces are acting on the shoulder. These forces can damage the cartilage of the growth plate and play a role in the development of Little League shoulder. The only way to remove the stress and allow the injury to heal is to stop throwing. The longer players throw with arm pain, the longer the pain will last.
Therefore, the initial treatment plan for Little League shoulder always consists of rest from throwing. This period lasts 2 to 4 months. The pain usually resolves within the first month of rest. However, premature return to throwing often leads to the recurrence of pain. About 25% of injured players experience a recurrence of pain within 6 months of resuming throwing because they return too soon.
#3 Begin Physical Therapy for Little League Shoulder
Physical therapy is initiated early to normalize shoulder range of motion and to begin a progressive strengthening program. Side-to-side shoulder differences in arm rotation range of motion contribute to shoulder pain and the occurrence of Little League Shoulder. Physical therapists evaluate athletes with Little League Shoulder to address these risk factors. The cross-body stretch is one exercise that targets posterior shoulder tightness, which contributes to loss of motion in overhead athletes.
Strengthening the rotator cuff and shoulder blade muscles is important to build arm strength while resting from throwing. Rotator cuff weakness is a risk factor for shoulder and elbow injury in adolescent pitchers. Youth baseball players who do not demonstrate full pain-free strength of the rotator cuff muscles should not return to throwing. Sidelying external rotation and prone horizontal abduction exercises target the posterior rotator cuff muscles. These are typically weak in young throwers. It is also important for athletes to strengthen the lower body and core musculature. Weakness in these areas results in increased stress transferred to the throwing arm.
#4 Complete a Return to Throwing Program
Structured interval throwing programs allow for a safe transition back to play. These programs replicate game conditions progressively and safely. Individual differences exist. Programs are tailored to the injured athlete’s physical and emotional needs.
Rushing the throwing program will lead to a recurrence of symptoms and a delayed return to play. Also, early long toss throwing should be progressed slowly due to increased rotational forces imposed on the healing growth plate. Communication between the medical team and coaching staff is important to ensure the success of the interval throwing program.
#5 Correct Flaws in Pitching Mechanics Before Returning to Play
Before returning to unrestricted play, injured athletes should have their throwing mechanics assessed by their coach. In particular, the rate of trunk and pelvis rotation during the acceleration phase of throwing has been linked to shoulder injuries in youth baseball players.

Hip-to-shoulder separation refers to the position of the hips relative to the shoulder just before the front foot contacts the ground. With ideal pitching mechanics, the hips are facing home plate, and the shoulder continues to face towards third base in a right-handed pitcher. This allows for the optimal transfer of force from the core to the throwing arm. As fatigue increases, the hips and shoulder begin to rotate in unison, resulting in an open hip-to-shoulder separation. The loss of power generation results in increased stress placed upon the shoulder and elbow. To reduce shoulder stress, this flaw must be corrected.
Rehab From Little League Shoulder
Little League Shoulder usually resolves with 3-4 months of rest, but symptom recurrence may occur. It is important to not rush back to throwing before range of motion and strength have returned. Correcting pitching mechanic flaws and a progressive throwing program is also required before fully returning to play.
Even after returning to play, close monitoring of athletes for at least 1 year is recommended to ensure the prevention of recurrence. Finally, current guidelines regarding pitch counts, rest, and activity modification should continue to be emphasized for long-term health.
If your youth athlete is experiencing symptoms of Little League Shoulder, contact your doctor or physical therapist. Parents, coaches, and the medical team will work together to guide the young baseball player back to 100%.
